Hair Loss in Your 50s and 60s: Is It Too Late for Hair Restoration?
The question arrives in the consultation room with a particular kind of resignation attached to it.
Not the panic of a twenty-something watching his hairline move. Not the frustration of a thirty-five-year-old managing progressive loss through the prime of his career. Something quieter and more settled — a man in his fifties or sixties who has been living with significant hair loss for years, sometimes decades, and who has arrived at the point of asking whether anything can still be done about it.
The assumption underneath that question is usually that the answer is no. The window has closed. That hair restoration is something for younger men, and that having waited this long — whether by choice, by circumstance, or simply by not knowing the options existed — means the decision has been made by default.
That assumption is wrong in most cases. And understanding why it’s wrong — what actually changes about hair restoration in the second half of life, and what doesn’t — is the most useful thing a man in this situation can have before he decides the question isn’t worth asking. Contact Northwestern Hair Restoration today for more information.
Where the Assumption Comes From
The belief that hair restoration is a young man’s domain isn’t random. It has a few sources that are worth identifying before dismantling them.
The most visible hair restoration marketing skews young. Before-and-after content tends to feature patients in their thirties and early forties. The cultural conversation about hair loss — the products, the procedures, the forums — centers on men at the beginning of their hair loss journey, not the men who’ve been living with the outcome for twenty years.
There’s also a general cultural association between cosmetic procedures and youth — the idea that interventions intended to improve appearance are more appropriate, more accepted, and more legitimate for younger people pursuing them than for older ones. This association is worth examining and discarding because it doesn’t reflect clinical reality, and it doesn’t serve patients.
And there’s a practical concern that’s more legitimate but still frequently overstated: the worry that significant loss combined with older age means there’s nothing meaningful left to work with. That the donor supply is inadequate, the remaining hair too thin, the scalp too changed by decades of loss to support a good outcome.
Each of these concerns has a clinical dimension worth addressing honestly. None of them constitutes a general disqualification for hair restoration in your fifties and sixties.
What Actually Changes With Age
 To answer the question of whether it’s too late, you have to understand what age actually changes about the hair restoration equation — and what it doesn’t.
To answer the question of whether it’s too late, you have to understand what age actually changes about the hair restoration equation — and what it doesn’t.
The Loss Pattern Is Often Stable
This is the most significant clinical advantage of addressing hair loss in your fifties and sixties that most patients don’t anticipate.
The aggressive, active progression that characterizes hair loss in the twenties and thirties — the rapid advance of the Norwood pattern that makes surgical planning difficult because the endpoint isn’t yet knowable — has typically reached its conclusion by the time a man is in his mid-fifties. The loss pattern he’s living with at 55 or 60 is, in most cases, close to the pattern he’ll have at 70. The trajectory has landed.
This stability changes the surgical planning equation fundamentally. The concern that drives caution in younger patients — that operating on the current state means designing around an incomplete picture — is largely resolved in older patients. The canvas is known. The full extent of loss is visible. The donor supply that exists is the available donor supply, and it can be allocated with confidence rather than held in reserve against a future that’s now more predictable.
A surgeon designing a procedure for a 57-year-old knows what they’re working with in a way that the same surgeon designing a procedure for a 27-year-old does not. That certainty is a clinical asset, and it makes the older patient in some ways a more straightforward surgical planning case than the younger one — not despite the advanced loss, but partly because of it.
DHT Levels Have Moderated
As discussed in the biology piece earlier in this series, DHT levels and 5-alpha reductase activity both tend to decrease somewhat with age. The hormonal pressure driving follicular miniaturization in the fifties and sixties is generally lower than it was in the thirties and forties.
For transplanted follicles — which carry DHT resistance from the donor area regardless — this hormonal moderation is irrelevant. But for the native hair that surrounds and exists alongside the transplant, a reduced hormonal environment means the progression of loss in areas not treated surgically tends to be slower. The ongoing maintenance challenge that makes younger patients’ results more complex to manage over time is somewhat less acute in older patients.
This doesn’t mean native hair stops thinning in your fifties. It means the rate of progression has typically slowed, which makes the overall management picture more stable and the long-term trajectory of a transplant result more predictable.
General Health Becomes a More Active Variable
The surgical candidacy question has a medical dimension in older patients that is less prominent in younger ones. Elective surgical procedures require physiological resilience — adequate healing capacity, absence of conditions that affect anesthetic response or post-operative recovery, medications that don’t interact problematically with the procedural environment.
For most healthy men in their fifties and sixties, these factors don’t constitute barriers. Hair transplantation under local anesthesia is a low-risk procedure with a well-established safety profile. The physical demands of the recovery are minimal. The healing capacity required is modest. Men in good general health at 55 or 65 are not categorically different from men at 40 from a surgical risk standpoint.
What changes is the importance of the pre-consultation medical history. Conditions that are managed with background variables in a 35-year-old — controlled hypertension, anticoagulant medications, thyroid regulation — deserve explicit attention in a 60-year-old because they’re more likely to be present and because their interaction with the procedure needs to be understood and managed rather than assumed away.
A thorough consultation at Northwestern Hair addresses this directly. The goal isn’t to create barriers to surgery for older patients — it’s to ensure that the procedure is designed around the patient’s complete clinical picture, which at 60 typically includes more variables than it does at 35.
Skin and Scalp Changes
Scalp skin changes with age in ways that are clinically relevant for both surgical execution and result quality.
Skin loses collagen and elasticity over decades, which can affect healing time and the character of the scalp surface post-procedure. Scalp laxity — the looseness of the scalp relative to the underlying tissue — tends to change with age in ways that affect how the donor area looks and feels after extraction. Blood supply to the scalp changes modestly with age as vascular aging progresses.
None of these changes is disqualifying. They’re variables that inform how the procedure is approached — the extraction technique used, the placement strategy, the post-procedure care protocol. A surgeon with experience across a range of patient ages manages these variables as part of normal clinical practice rather than treating them as obstacles.
What skin aging doesn’t change is the fundamental biology of transplanted follicles. DHT-resistant follicles moved from the donor area to the recipient site, and grow in a 60-year-old scalp by the same mechanism as they grow in a 30-year-old scalp. The permanence of the transplant isn’t contingent on the age at which it’s performed.
The Donor Area Question at 60
The concern that drives the most legitimate hesitation about hair restoration in older patients is donor supply — and it deserves direct engagement rather than reassurance.
A man who is 60 with Norwood Stage 6 or 7 loss has more recipient area to cover and, in some cases, a donor area that has itself changed over the decades. In the most challenging presentations — patients with naturally low donor density, hair loss that has extended into the donor zone, or prior procedures that consumed significant donor supply — the available grafts may genuinely not support the coverage the patient is hoping for.
This is a real limitation. It’s not a reason to avoid the consultation — it’s precisely the reason to have it. The question isn’t whether donor supply is theoretically sufficient for the ideal outcome. It’s whether the available supply, allocated intelligently to the areas where coverage makes the most functional and aesthetic difference, produces a result that meaningfully improves the patient’s situation.
For most patients in their fifties and sixties, the answer is yes. Even in advanced loss cases, strategic allocation of available grafts — prioritizing the hairline and frontal zone, which carry the most visual weight and the most impact on perceived age and vitality — can produce results that significantly improve how a patient presents to the world, even when comprehensive coverage of the full thinning zone isn’t achievable in a single procedure.
The specific techniques Northwestern Hair has developed for managing extensive cases — ACS donor preparation to increase blood flow and tissue strength, iso-hypothermal plasmonic preservation to maintain graft viability during long procedures, sequential extraction to target specific graft types needed for the recipient zone — expand what’s achievable even when donor supply is the primary constraint. These aren’t workarounds for a difficult situation. They’re precision tools that make difficult cases genuinely more manageable.
What Results Look Like for Older Patients
The naturalness standard — the goal of a result that reads as hair rather than procedure — is if anything more achievable in older patients than in younger ones, for a specific reason.
The hairline appropriate for a 58-year-old is not the hairline appropriate for a 28-year-old. It sits slightly higher. It has a mature character. It fits the face in a way that is calibrated to the patient’s actual age rather than to the youth of a design template. And because the surgical goal isn’t to recreate the hairline of someone’s twenties but to restore something natural and age-appropriate, the design has more room to breathe — more latitude to create something that looks genuinely right rather than conspicuously restored.
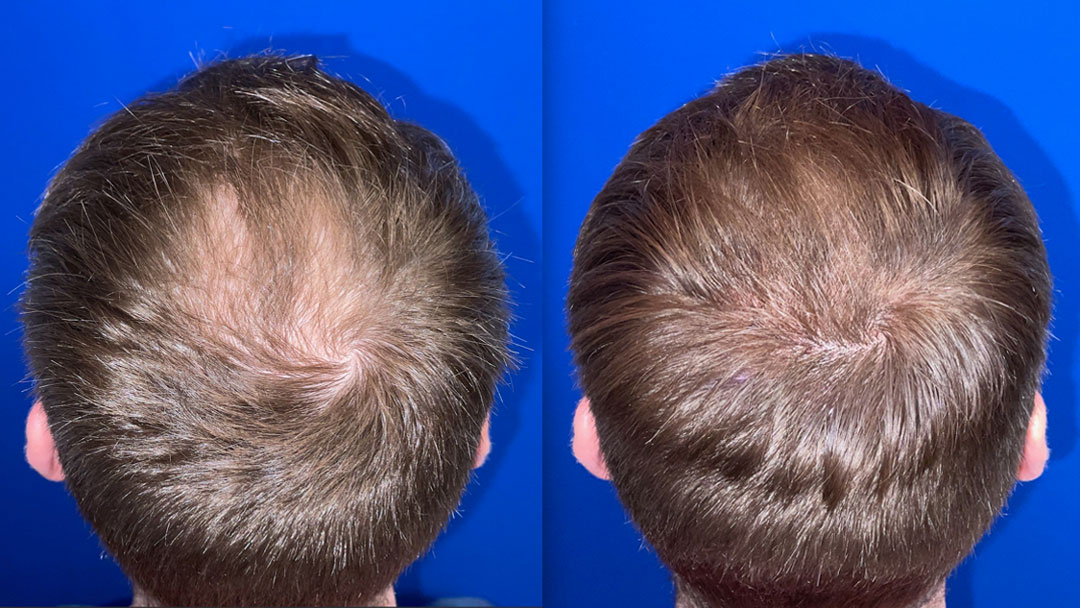
The before-and-after transformation in older patients is also, in many cases, more dramatic in impact than the equivalent change in a younger patient — not because the result is more extensive, but because the relationship between appearance and perceived age and vitality is more pronounced. A 55-year-old who looks ten years younger as a result of restored frontal density is experiencing a more significant quality-of-life change than a 30-year-old whose already-early hairline recession is refined.
This is something patients in this age group often don’t anticipate going into the consultation. They’ve been living with the loss for long enough that they’ve partially adjusted their self-image to accommodate it. The gap between that adjusted self-image and the result — the first time they see themselves at the eight or nine month mark with density returning — tends to produce a more pronounced response than the clinical description of the change would suggest.
Non-Surgical Options Remain Relevant
Not every patient in their fifties and sixties will choose surgery, or be the right candidate for it. For these patients, non-surgical treatment at this stage of hair loss is a different proposition than it is for younger patients, but it isn’t irrelevant.
ACS for Older Patients
The population of miniaturized follicles that ACS targets — follicles that are present and compromised but not yet permanently lost — still exists in many patients with significant long-standing loss. Areas of thinning rather than full baldness, zones of visible density reduction rather than complete absence, regions where the scalp surface has hair present but insufficient to provide cosmetic coverage — these are areas where regenerative treatment can still produce meaningful improvement.
For an older patient who either isn’t a surgical candidate or who wants to improve the non-transplant areas alongside or instead of surgery, ACS represents a genuine clinical option. The goals are different than in a twenty-something — not prevention of future loss, but improvement of what’s present and maintenance of what remains. But the mechanism is the same, and the biological responsiveness of miniaturized follicles doesn’t expire at a specific age.
SMP as a Standalone or a Complement
Scalp Micropigmentation is particularly relevant for older patients who want visual density improvement without surgery. For the patient with a shaved or very close-cropped head, SMP can create the appearance of fuller coverage by simulating the look of closely cut follicles across the thinning zones. For the patient with longer hair, SMP adds visual density between existing hairs in a way that photographs well and reads as natural at social distances.
As a complement to a surgical result in an older patient where donor supply constraints limit full coverage, SMP addresses the zones that grafts couldn’t reach — creating a cohesive overall picture rather than leaving a visible contrast between the transplanted front and the uncovered posterior zones.
The Professional and Life Context
One dimension of hair restoration in your fifties and sixties that differs meaningfully from earlier decisions is the professional and personal context surrounding it.
Men at this stage of life are often at or near the peak of their professional visibility — senior leadership roles, client-facing responsibilities, public or community profiles that make appearance more consequential in certain ways than it was at 35. The motivation to address hair loss isn’t vanity in the pejorative sense. It’s the same attention to professional presentation that leads anyone in a high-visibility role to manage every aspect of how they show up.
The discretion considerations are also different. A man in his fifties taking a few days off for a medical procedure raises fewer eyebrows than a younger colleague doing the same. The professional calendar tends to be more within his control. The social awareness that made recovery feel conspicuous at 30 has largely been replaced by the confidence to simply manage the logistics without extensive explanation.
The recovery itself is the same regardless of age — the same ten-day active window, the same twelve-month growth arc, the same post-procedure protocol. The professional and personal context for managing that recovery at 55 is, in most cases, considerably more accommodating than it was two decades earlier.
When It Actually Is Too Late
Honesty requires acknowledging the scenarios where the answer to “is it too late” is genuinely yes — or at least yes for surgery.
A patient with diffuse loss that has extended into the donor zone — where the follicles at the back and sides of the scalp have themselves miniaturized significantly — may not have adequate DHT-resistant donor supply to support a meaningful procedure. The permanence of the transplant depends on the DHT resistance of the donor follicles. If those follicles are themselves vulnerable, the transplant isn’t permanent in the way it needs to be.
A patient with serious uncontrolled medical conditions — poorly managed cardiovascular disease, anticoagulation requirements that can’t be temporarily modified, conditions that significantly impair healing — may not be an appropriate surgical candidate until those conditions are better controlled. This is a timing issue rather than a permanent disqualification in most cases, but it requires honest medical evaluation before surgery is appropriate.
A patient with expectations that the available donor supply cannot support — seeking full density coverage of extensive loss with a donor area that can’t deliver it — isn’t someone surgery will satisfy regardless of technical execution. The right response in this scenario is the same as it is at any age: an honest conversation about what is achievable, and a decision made from that honest picture rather than from unrealistic expectations.
These scenarios are real. They’re also not the majority of patients in their fifties and sixties who walk through the consultation door. For most, the clinical picture supports a meaningful, natural-looking result from a well-designed procedure — and the only thing genuinely standing between them and that result is the assumption that the question isn’t worth asking.
What the Fifties and Sixties Patient Has That the Twenty-Something Doesn’t
It’s worth ending this piece with a reframe that most men in this age group haven’t considered.
The patient is in their fifties and sixties, considering hair restoration isn’t behind the curve. In several clinically significant ways, they’re in a better position than the younger patient who acts from urgency.
Their loss pattern is known. The trajectory has completed its most unpredictable phase. The surgical plan can be designed with confidence rather than educated guesswork about where the loss will eventually end up.
Their expectations are calibrated by lived experience rather than shaped by anxiety. The man who has been living with hair loss for twenty years has a more realistic and more settled sense of what he wants from restoration than the twenty-three-year-old who hasn’t yet separated the emotional urgency from the clinical decision.
Their life context supports the decision. The professional autonomy, the personal confidence, and the financial position of a man at this stage of his career make the logistics of the procedure and recovery more manageable than they were at earlier stages.
And their goals are specific and achievable. They’re not asking for the hair of their twenties. They’re asking for something that looks appropriate, natural, and genuinely better than the alternative, which is exactly the kind of goal that a well-executed hair transplant at any age delivers best.
None of that makes hair restoration the right answer for every patient in their fifties and sixties. What it makes clear is that the question deserves to be asked — properly, honestly, and in a consultation room rather than dismissed before it gets there.
The Answer to the Question
Is it too late?
For most men in their fifties and sixties who are in reasonable general health, have not depleted their donor supply through prior procedures, and are carrying realistic expectations about what age-appropriate restoration looks like — no. It isn’t.
The biology that makes hair transplantation work doesn’t have an expiration date. The permanence of DHT-resistant follicles doesn’t diminish with the age of the patient they’re transplanted in. The natural aging of a well-executed result — graying gradually, maturing in texture, integrating with the rest of the scalp — is, if anything, more seamless in an older patient whose surrounding hair is going through the same changes.
What’s required is the same thing it’s always required: the right diagnosis, the right technique, the right surgical plan designed around the actual clinical picture rather than a template, and the right surgeon willing to have an honest conversation about what that picture supports.
That conversation is available regardless of how old you are when you finally decide to have it.
In your fifties or sixties and wondering whether you’ve waited too long? Book a consultation with Dr. Vinay at Northwestern Hair. The answer is probably not what you’re expecting.